What happens after "no further action"
- Shounak Bhattacharjee
- May 9
- 6 min read
On the quiet decisions we make at the end of a crisis assessment — and what they ask of the person on the other end of the line.
In crisis mental health work, one of the most common decisions isn't the dramatic one. It's the quiet one. The assessment ends, the risk is judged not to meet threshold for admission or further intervention, and the outcome is recorded as something close to "no further action" — signposting, self-help, a number to call back if things change.
I've been working in NHS crisis services for just over three years now, in one of the busiest mental health trusts in the country. Most of what I'm describing here is something I've sat with on the other end of a phone or a face-to-face assessment, not something I've read about. That matters, because the parts of this work that are hardest to write about are also the parts that don't show up in audits.
On paper, "no further action" is a normal clinical decision. Most assessments end this way. They have to. Services are finite, beds are finite, and most people in distress are not, in that moment, in immediate danger. Threshold judgements are part of how the system functions.
But something happens in the gap between the decision being made and the person hearing it. And that gap is where I've been paying attention.
What "low risk" sounds like from the other side
When a clinician says someone is at low risk, they usually mean something quite specific: the available information, weighed against structured frameworks and clinical judgement, doesn't point towards imminent harm. It's a probabilistic statement, made under time pressure, with partial information.
When a service user hears it, the meaning can be different. "Low risk" can sound like you are not serious enough. "No further action" can sound like we are not going to help. "Self-refer if things change" can sound like you are now alone with this.
That mismatch is rarely about miscommunication. People in distress are usually listening carefully. The mismatch is structural. The clinical framework is built around what the service can offer. The person's framework is built around what they're carrying.
When those two don't line up, the person doesn't usually argue. They go quiet. They thank the practitioner. They hang up. And the case is closed.
What the evidence actually says
The window immediately after contact with crisis services is one of the highest-risk periods in mental health care. The evidence on this is not new and not contested. Self-harm and suicide rates in the days and weeks following discharge from inpatient care, A&E mental health attendance, or crisis service contact are substantially elevated compared to the general population — particularly in the first week. (See Chung et al., 2017, JAMA Psychiatry, and the National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH) annual reports, University of Manchester.)
This isn't because the assessments were wrong. Most weren't. It's because risk isn't a stable property of a person. It moves. It responds to context — to what happened in the conversation, to what the person took away from it, to whether they felt heard, to what they're going home to.
A careful assessment that produces an accurate point-in-time judgement can still be followed by a deterioration the assessment couldn't have predicted. That's not a failure of clinical reasoning. It's the nature of the thing being assessed.
The question I keep returning to is whether our systems are designed around this fact, or around the more comfortable assumption that a sound assessment is the end of a clinician's responsibility.
Where the system quietly leans
In high-volume crisis services — and I work in one — there's pressure that isn't always explicit, but is always present, to bring assessments to a clean conclusion. A defensible outcome. A documented plan. A closed episode. These are not bad things. They make the work auditable and the service navigable.
But they also subtly reward a particular kind of ending. One where the clinician's risk has been transferred — to the person, to a self-referral pathway, to a future contact that may or may not happen. The episode closes. The dashboard updates. The work moves on.
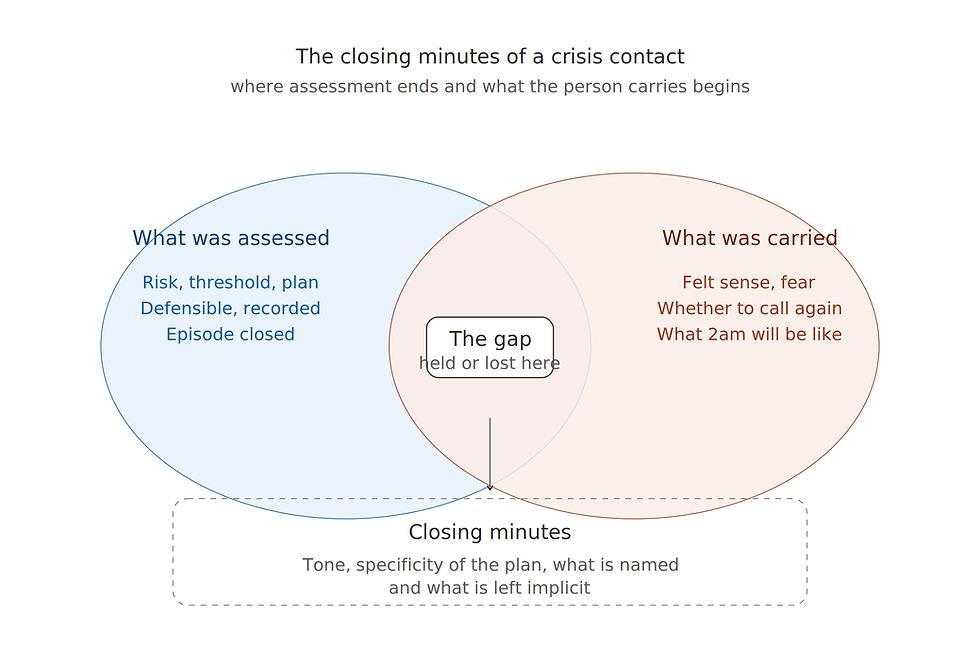
What's harder to see, and harder to measure, is what the person carried out of the conversation. Whether they felt their distress was understood, even if the response was constrained. Whether the safety plan was something they could actually use at 2am, or something they nodded along to because they wanted the call to end. Whether the next step — call back, see your GP, contact this service — felt like a real option or a polite dismissal.
These aren't soft questions. They are, in a real sense, the active ingredients of whether the assessment held.
What I am working towards
I'm not arguing for lower thresholds, or for admitting more people. Those are policy questions with their own trade-offs, and they can't be solved at the level of an individual call.
What I'm interested in is narrower. It's the texture of the closing minutes of a crisis assessment. The handful of decisions — what to say, what to write, what to follow up — that determine whether the person leaves the conversation with something useful, or with something that quietly confirmed the worst thing they suspected before they called.
After three years of doing this work, the thing I've come to trust least is the assumption that a defensible decision is the same as a sufficient one. They overlap, often. But not always. And the gap between them is rarely visible in the record.
Those minutes are doing more work than the system gives them credit for. And because they're hard to measure, they're often the first thing that gets compressed when services are under load.
Noticing that — and protecting it — feels like one of the more useful things behavioural science can offer to crisis care right now.
Practitioner Tool
A reflection set for closing a crisis contact
These prompts aren't a replacement for safety planning frameworks or trust-specific protocols. They're a way of slowing down the last few minutes of a contact, where a lot of the post-assessment risk lives.
What is this person likely to remember from this conversation in six hours?
Not the clinical content. The felt sense. Did they leave with something to hold onto, or with confirmation that they shouldn't have called?
Draws on: episodic memory under stress, affect-as-information, therapeutic alliance.
Is the safety plan written for this person, or for the record?
A plan that lists generic numbers and generic strategies tends to read as procedural. A plan that names something specific to them — a person, a place, a time of day they tend to struggle — tends to be used.
Draws on: implementation intentions, specificity effects in behaviour change.
What's the realistic probability they will use the next-step pathway I'm offering?
Self-referral routes have known drop-off. If someone is in distress now, the cognitive cost of initiating a new contact later is non-trivial. What would lower that cost?
Draws on: friction effects, intention-action gap, behavioural economics of help-seeking.
Am I closing this episode, or are they?
There's a difference between a contact that ends because the work is done, and one that ends because the form has a box to tick. The person can usually tell.
Draws on: procedural justice, perceived voice, service-user experience research.
If this person deteriorates tonight, what would the record show I considered — and what would it miss?
Not as a defensive exercise, but as an honest one. The gap between what's documented and what was actually weighed up is often where learning lives.
Draws on: reflective practice, hindsight bias, post-incident review literature.
What did I not have time to do that I would have wanted to?
Naming the constraint is part of the work. It separates the limits of the assessment from the limits of the person's situation, which the system tends to conflate.
Draws on: moral injury, system-level honesty, distinction between constraint and consent.
Measurement and protocol will always be necessary in crisis services. The question isn't whether to use them, but whether the closing minutes — the part that holds most of the post-contact risk — are being given the attention the evidence says they deserve.


Comments